|
Prior to 1985, minimal incision hallux abducto valgus (HAY) corrective procedures available to the podiatric surgeon, with the exception of a Wilson bunionectomy, although highly effective, were a compromise and failed to take into consideration the importance of the proximal articular set angle. An increased proximal articular set angle in the HAV deformity results in instability of the MPJ and increased structural and positional forces that increase the first intermetatarsal angle and the hallux abductus angles. Architect Maurice Amado, an expert structural consultant, confirmed the importance of the PASA in HAV formation and the need to reduce this angle in hallux abducto corrective surgery (personnel communication, University of Idaho, 1989). From a structural viewpoint, a joint that is straight on the metatarsal bone is much more stable than one that is at an angle (Fig. 4).
 
Figure 4
- Preoperatibe view of a patient with PASA deformity.
- The same patient 2 years after an unsuccessful modified McBride-Akin procedure. The surgery failed to correct PASA.
- The successful correction of the PASA with the Isham osteotomy can be seen in this radiograph taken 5 years after surgery.
In the early 1980s, I had a goal to perfect a bunionectomy procedure that used the modern and highly effective advances of the ambulatory podiatric surgeons. Using minimal incision techniques, Reverdin bunionectomies were performed. These minimal incision Reverdin bunionectomies proved to be superior to previously used procedures in the correction of the involved structural and positional components of HAV disorders. As with the large incision Reverdin bunionectomy procedures, in which a medial wedge osteotomy was performed through the first metatarsal head dorsal to planter perpendicular to the weight-bearing surface of the first metatarsal, degenerative joint disease resulted when the osteotomy was placed through the articular surface on the planter aspect of the head of the first metatarsal. The osteotomy interfered with the normal function of the sesamoid bones, resulting in decreased range of motion at the MPJ.
The author modified the Reverdin osteotomy with the Isham osteotomy by performing the medial wedge osteotomy in the head of the first metatarsal at an angle from dorsal distal, just proximal to the articular surface on the dorsal aspect of the head, to planter proximal to a point just proximal to the articular surface on the planter aspect of the first metatarsal head (Figs. 5, 6, and 7).
 |
|
|
Figure 5
The Reverdin-Isham procedure.
- A dorsoplantar view demonstrating the portion of the medial eminence resected and the level at which the osteotomy is performed.
- The same view showing the wedge of bone resected to achieve correction.
- The correction is made with the arrow showing the direction of closure.
- A medial view of the first metatarsal demonstrating the plantar-medial incision, the capsulotomy, and the placement of the bone cutting instrument prior to the osteotomy.
- After the removal of the wedge and before closure.
- The completed osteotomy after closure and correction of the structural deformity.
|
| |
 |
|
|
Figure 6
- The dorsoplantar view of an osteotomy site.
- The medial view of an osteotomy site.
|
| |
 |
|
|
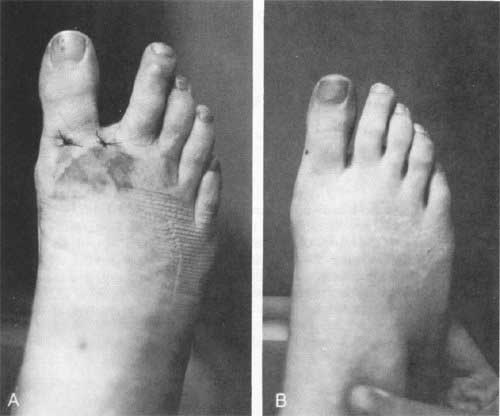
Figure 7
The clinical appearance of the foot
- after 2 days and
- after 3 months.
|
This placement of the Isham osteotomy preserves and repositions the articular surface, corrects the proximal articular set angle, and redirects and stabilizes the structural forces at the first metatarsophalangeal head. The placement of the osteotomy inside the joint capsule in the cancellous bone of the first metatarsal head proved to be highly stable and eliminated the need for internal fixation. As hoped, the postoperative management proved to be the same as is needed for the minimal incision Silver-Akin procedure or modified McBride-Akin. No increased pain or disability was noted. Marked improvement of short- and long-term results were immediately apparent.
|
