| |
ISHAM HAMMERTOE PROCEDURES FOR THE CORRECTION OF LESSER DIGITAL DEFORMITIES
PHALANGEAL OSTEOTOMY PROCEDURES
By Stephen A. Isham, DPM, MD
Photos: Dr. Pau Golano and Dr. M DePrado
Art: Dr. S. Isham
|
| |
Introduction |
|
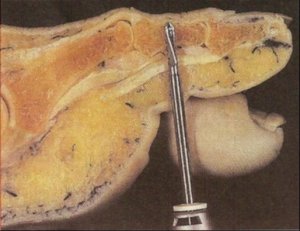
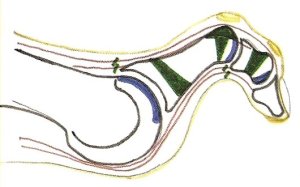
The surgical procedures presented are for the treatment of a variety of hammertoe deformities by performing combination or wedge osteotomies in the proximal or medial aspect of the phalange preserving the articular surfaces of the phalangeal joints resulting in a correction of the structural deformity of the lesser digits. The Isham Hammertoe Procedures with pre operative criteria, techniques of operation, advantages and disadvantages are presented.
|
| |
Definition |
|
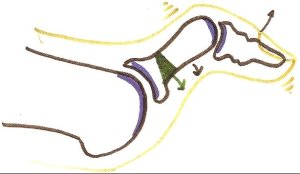
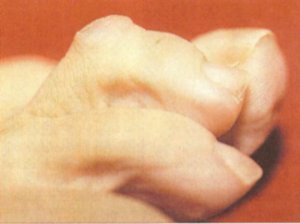
Hammertoe deformities are a combination of one or more deformities of the digits on the metatarsal phalangeal joints. These deformities can be in the saginal, transverse, and frontal planes. Most commonly, the deformed digit is dorsal flexed at the metatarsal phalangeal joint and plantarflexed at the interphalangeal joints or distal phalangeal joints. These deformities contain both soft tissue and osseous components called positional and structural deformities.
|
| |
Etiology |
|
One of the most common manifestations of biomechanical functional abnormalities of the foot is expressed in painful deformities of the lesser digits. This manifestation can be expressed by soft tissue and structural components caused by normal adaptive changes on soft tissue and osseous structures. Digital deformity can occur at the MPJ joint, the proximal IPJ joint, and the distal IPJ joint of the involved digit.
The primary cause of hammertoe deformities is the abnormal foot structure which, as dictated by genetic code, is exposed to abnormal pronatory forces resulting in hypermobility of the osseous structures and over dependence on soft tissue structure for stability during weight bearing and in particular during the last phase of the propulsive stage of gait. The severity of the hammertoes is proportionate to the severity of the abnormal pronatory forces present. Other causes of hammertoe deformities are systemic diseases such as gout, rheumatoid arthritis, neurological disorders, or trauma causing permanent osseous or soft tissue damage to the digit. Footwear, though not a primary cause, can aggravate the symptoms of the deformity.
|
| |
Classification |
|
The classification of deformities is an instrument to enable the surgeon to select modifying procedures to achieve its best result for each patient. To classify the severity of hammertoe deformities, the following observations are commonly used by the author. These observations are related to the percentage of soft tissue versus osseous adaptive deformities. They are flexible, semi-flexible, semi-rigid, and rigid.
The aim of the Isham Hammertoe Procedures is directed at correcting the soft tissue structures by doing soft tissue releases of the extensor and flexor tendons and a capsulotomy at the metatarsal phalangeal joint, if indicated, and correcting the structural deformities while conserving the articulation and utilizing the adaptive changes that are occurring at these joint structures. By using these conservative osteotomy and soft tissue procedures, we can redirect the biomechanical function and improve the appearance and symptoms of the deformed digit.
Most deformed digits that we are called upon to correct have been long term enough to have both components, structural and soft tissue abnormalities. The components of the deformity is the result of adaptive changes taking place at the involved joint or joints of the digits. The longer the contracture of the digit the more osseous adaptive changes will occur.
Development of surgical procedures is an evolution based on the work of previous surgeons. Diaphyseal osteotomy procedures of the phalanx have been utilized for years for the correction of hammertoe deformities. The author has modified these procedures by using a combination, and wedge osteotomies at the base of the proximal phalanx, in conjunction when indicated with a combination osteotomy of the middle phalanx and a wedge osteotomy when indicated along with exostectomies and soft tissue corrections.
|
| |
Phalangeal Osteotomy Procedures |
|
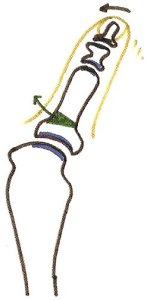
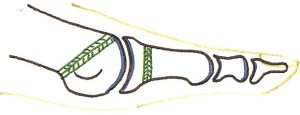
Wedge osteotomy is an osteotomy procedure where a wedge is performed in the diaphysis or metaphysis whereby a cortical or periosteal hinge is conserved redirecting or realigning the osseous structures on an anatomical guideline.
Combination osteotomy is an osteotomy procedure in the diaphysis or metaphysis of the bone where a transverse bone shortening osteotomy is performed through the cortex and periosteum but also wedged to realign the osseous structures and improve function.
|
| |
Isham Hammertoe Procedures |
|
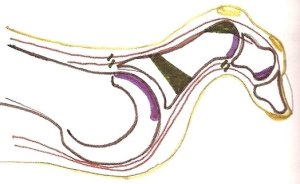
I-1 procedure. This procedure is a combination osteotomy at the base of the proximal phalanx with soft tissue releases of the two extensor and flexor tendons and, if necessary, a capsulotomy on the dorsal aspect of the metatarsal phalangeal joint. This procedure is indicated in a semi-flexible hammertoe deformity where a majority of the deformity takes place at the MPJ joint.
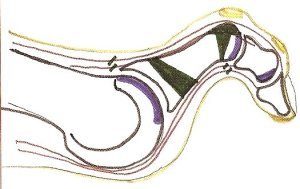
 I-2 procedure. This procedure is a combination osteotomy performed at the base of the proximal phalanx and an exostectomy performed on the dorsal aspect of the head of the proximal phalanx along with extensor and flexor soft tissue releases. This is indicated for a semi-flexible hammertoe deformity with an exostosis on the head of the proximal phalanx.
I-2 procedure. This procedure is a combination osteotomy performed at the base of the proximal phalanx and an exostectomy performed on the dorsal aspect of the head of the proximal phalanx along with extensor and flexor soft tissue releases. This is indicated for a semi-flexible hammertoe deformity with an exostosis on the head of the proximal phalanx.
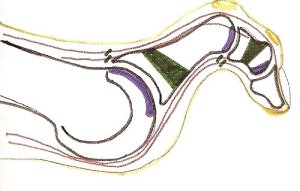
 I-3 procedure. This procedure is a combination osteotomy at the base of the proximal phalanx, an exostectomy on the dorsal aspect of the head of the proximal phalanx, and a dorsal wedge osteotomy through the head of the proximal phalanx with extensor and flexor soft tissue releases resulting in a realignment and straightening of the articular surface of the proximal IPJ. This is indicated for a semi-rigid deformity with a long phalanx with a deformity at the MPJ and PIPJ.
I-3 procedure. This procedure is a combination osteotomy at the base of the proximal phalanx, an exostectomy on the dorsal aspect of the head of the proximal phalanx, and a dorsal wedge osteotomy through the head of the proximal phalanx with extensor and flexor soft tissue releases resulting in a realignment and straightening of the articular surface of the proximal IPJ. This is indicated for a semi-rigid deformity with a long phalanx with a deformity at the MPJ and PIPJ.
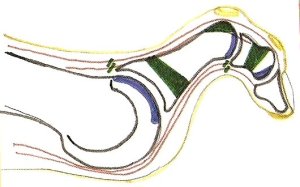
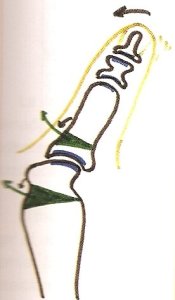
 I-4 procedure. This procedure is a combination osteotomy at the base of the proximal phalanx and a combination osteotomy procedure in the diaphysis of the middle phalanx with associated extensor and flexor releases. This is indicated for semi-flexible hammertoe deformity where the deformity is not only at the MPJ but also at the proximal and distal IPJ joints. The deformity at the proximal IPJ joint is reducible by the soft tissue releases. This procedure is the most common hammertoe procedure utilized by the author.
I-4 procedure. This procedure is a combination osteotomy at the base of the proximal phalanx and a combination osteotomy procedure in the diaphysis of the middle phalanx with associated extensor and flexor releases. This is indicated for semi-flexible hammertoe deformity where the deformity is not only at the MPJ but also at the proximal and distal IPJ joints. The deformity at the proximal IPJ joint is reducible by the soft tissue releases. This procedure is the most common hammertoe procedure utilized by the author.
 I-5 procedure. This procedure is a combination osteotomy at the base of the proximal phalanx and an exostectomy at the hypertrophied exostosis on the dorsal aspect of the proximal phalanx and a combination osteotomy of the middle phalanx. This is indicated for a semi-rigid deformity of the digit which exists at the MPJ and the IPJ�s with exostosis on the dorsal aspect.
I-5 procedure. This procedure is a combination osteotomy at the base of the proximal phalanx and an exostectomy at the hypertrophied exostosis on the dorsal aspect of the proximal phalanx and a combination osteotomy of the middle phalanx. This is indicated for a semi-rigid deformity of the digit which exists at the MPJ and the IPJ�s with exostosis on the dorsal aspect.
 I-6 procedure. This procedure is a combination osteotomy at the base of the proximal phalanx, an exostectomy on the dorsal aspect of the head of the proximal phalanx, a dorsal wedge osteotomy through the head of the proximal phalanx, and a combination osteotomy at the diaphysis of the middle phalanx. This is indicated for a rigid hammertoe deformity with multiple areas of deformity of the MPJ and the two IPJ�s in a long digit. This procedure is utilized mostly in a 2nd digit.
I-6 procedure. This procedure is a combination osteotomy at the base of the proximal phalanx, an exostectomy on the dorsal aspect of the head of the proximal phalanx, a dorsal wedge osteotomy through the head of the proximal phalanx, and a combination osteotomy at the diaphysis of the middle phalanx. This is indicated for a rigid hammertoe deformity with multiple areas of deformity of the MPJ and the two IPJ�s in a long digit. This procedure is utilized mostly in a 2nd digit.
|
| |
Non-Hammertoe Lesser Digit Deformities |
|
Digital deformities may be associated with a non-biomechanical abnormalities, such as congenital or acquired deformities. In a laterally or medially deviated digit the PASA is effected either positively or negatively at the metatarsal phalangeal joint. It is often noticed with hallux valgus deformities where the lesser digit is deviated also laterally or medially overlapping the hallux. This laterally deviated is very common in arthritic conditions such as rheumatoid arthritis.
 If the digital deformity is associated strictly with a deformity at the MPJ joint and there is no metatarsal deformity or a keratosis or symptomatology on the metatarsal, then a wedge phalangeal osteotomy may be performed to straighten out the digit. This procedure is performed without or in conjunction with soft tissue releases, as needed.
If the digital deformity is associated strictly with a deformity at the MPJ joint and there is no metatarsal deformity or a keratosis or symptomatology on the metatarsal, then a wedge phalangeal osteotomy may be performed to straighten out the digit. This procedure is performed without or in conjunction with soft tissue releases, as needed.
 A wedge osteotomy procedure may be performed to straighten out a laterally deviated or medially deviated digit in conjunction with a Modified Isham Osteotomy through the head or neck of the metatarsal correcting the PASA as well as elevating the metatarsal head for a painful lesion underneath the metatarsal head area. Again, soft tissue procedures are usually not performed, only when indicated.
A wedge osteotomy procedure may be performed to straighten out a laterally deviated or medially deviated digit in conjunction with a Modified Isham Osteotomy through the head or neck of the metatarsal correcting the PASA as well as elevating the metatarsal head for a painful lesion underneath the metatarsal head area. Again, soft tissue procedures are usually not performed, only when indicated.
On congenital deformities of the 5th digit, an overlapping 5th digit to the 4th digit has proven to be a challenge for many years to correct this deformity. This deformity may be corrected by doing a combination osteotomy at the base of the proximal phalanx in conjunction with an extensor tenotomy and capsulotomy releases. The correction is maintained by dressings for approximately six weeks versus the ten days to two weeks for other hammertoe deformities. On occasion should the adaptive cartilage of the 5th digit be significantly dorsal at the MPJ on the metatarsal head, that a combination osteotomy is needed on the metatarsal plantarly in order to re-position the adaptive cartilage more towards normal function position directly in front of the metatarsal head.
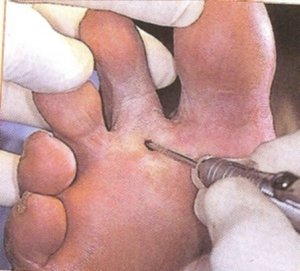
Exostosis excisions may be performed using percutaneous incisions on any hyperostosis on the phalanx such as on the distal aspect of the digit, at the distal IPJ, the proximal IPJ either dorsal or medial or lateral.
Congenitally long digit that has no deformity factors at either the IPJ or MPJ, a shortening osteotomy procedure may be performed in both the base of the proximal phalanx and in the middle phalanx without soft tissue releases in order to render the digit in its more normal length.

|
| |
Complications |
|
Limitation of flexion at the proximal IPJ occurs in approximately 20% of the procedures performed, this is associated with fibrous adhesions around the joint structures. These are almost always asymptomatic and do not interfere with normal function during gait.
Failure to adequately release the soft tissue structures may result in telescoping of the osseous segments at the osteotomy site. This will result in slower healing and possibly a malposition or malunion at the osteotomy site.
Fibrous union clinical fusion occurs quite rapidly in less than three weeks at the osteotomy sites however, due to the lack of highly vascularized soft tissue structures around the phalanx, bony ossification is approximately twice as long as with metatarsal osteotomies, this is an asymptomatic finding.
The goal of the procedure is to functionally realign the osseous segment not realign the osseous segments anatomically. Should symptomatic failure of the procedure occur, then a traditional or Minimal Invasive arthroplasty or partial head resection may be performed using percutaneous procedures.
|
| |
Summary |
|
Correction of lesser digital deformities using percutaneous procedures using exostectomy but primarily combination osteotomies with soft tissue releases correct the vast majority of digital pathology. These procedures are very conservative, however, should we have a rare failure, use of traditional hammertoe procedures would be a viable option. In most cases, a repetition or modification of the original Isham Hammertoe Procedure is effective.
|
| |
|
|
|